

Diagnosis: Merkel cell carcinoma
Description: Nodule selected for excision biopsy
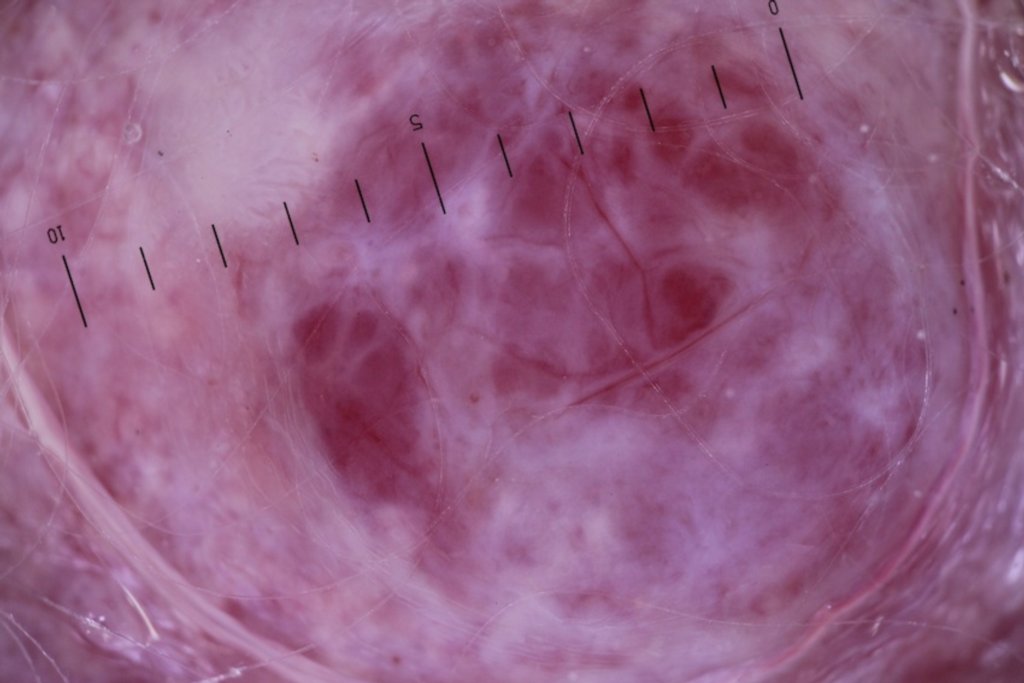
Morphology: Nodule pink
Site: Scalp
Sex: M
Age: 81
Type: Clinical & Histology
Submitted By: Ian McColl
Differential Diagnosis
History:
Case from Dr
| 81yo male (last seen 6/12 ago) presents for routine skin cancer examination and has noted a 2/12 history of growing nodules on his scalp. He visited his regular GP a few weeks earlier and mentioned them. His GP allegedly said that these lesions were benign and would need laser removal. Excision would bleed too much so, not worth doing.
PMhx: Well. Minimal medication. Increased PSA, monitored by Urologist only at this stage. Full systems review revealed no concerning symptoms with regards to sinister internal malignancies OE: Dermoscopically: featureless pink clods with white lines and white featureless areas. They were much more featureless than I had expected macroscopically. Haemangiomas in general have pink/red or purple clods mainly with limited white lines. General examination normal with head, neck or supraclavicular lymphadenopathy Imp: Fast growing pink nodules on a solar damaged scalp of an elderly gentleman. Dx: Merkels Cell Carcinoma I excision biopsied an entire nodule from the field for diagnosis. The diagnosis was 'strongly suggestive of Merkel Cell Carcinoma' and involved the entire specimen thickness and the margins. Mx: Urgent referral to radiation oncologist last week, booked plastic surgeon for wide margin excision with skin graft. PET scan today revealed no spread to organs at this stage. Will follow up in 3/12 after surgery and radiation treatment. Follow Up Clinical notes: Central scalp - Rapid growing large pink nodules x 3 in Macroscopic: The specimen consists of an ellipse of skin measuring 29 x 16 x 3mm bearing Microscopic: Sections show an undifferentiated small round cell malignancy which is SUMMARY:
Immunohistochemistry has been performed. The tumours cells are strongly and The immunohistochemical features are not completely specific but are most SUMMARY:
|