

Diagnosis: Disseminated superficial actinic porokeratosis
Description: Porokeratosis of Mibelli
Morphology: Red,scaly
Site: Limbs
Sex: F
Age: 70
Type: Clinical & Histology
Submitted By: Ian McColl
Differential Diagnosis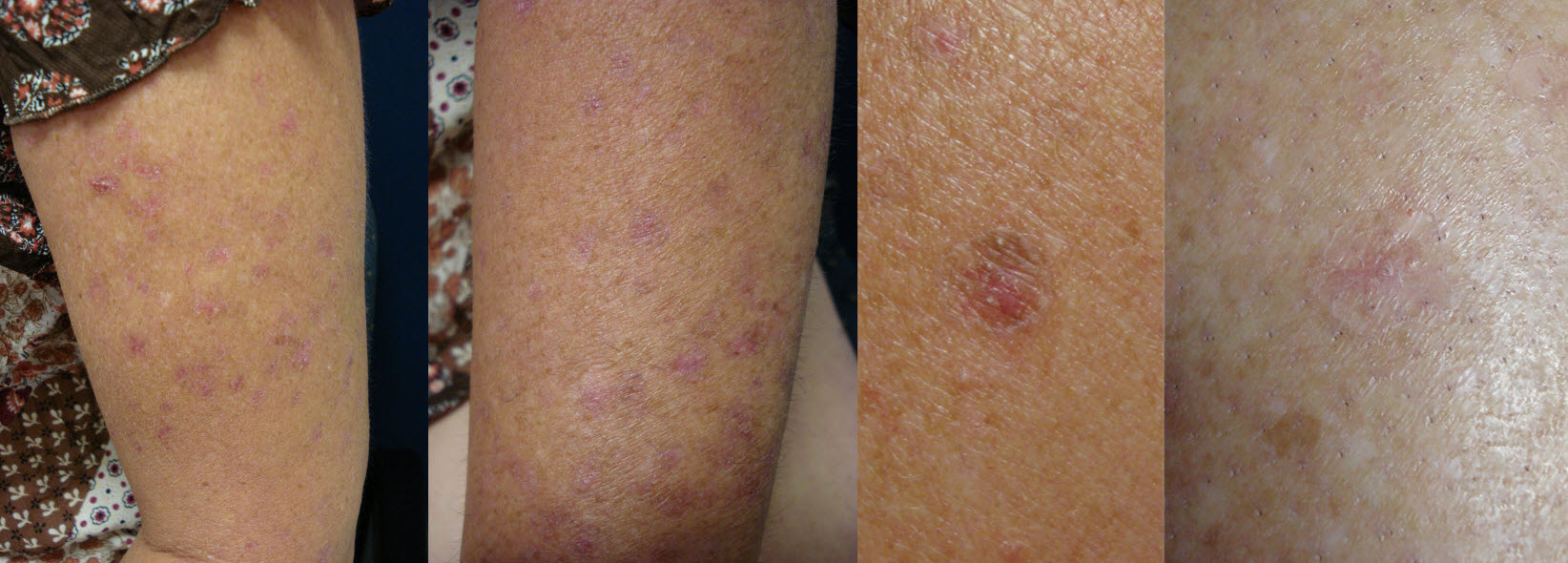
History:
| Case 2_G.C.
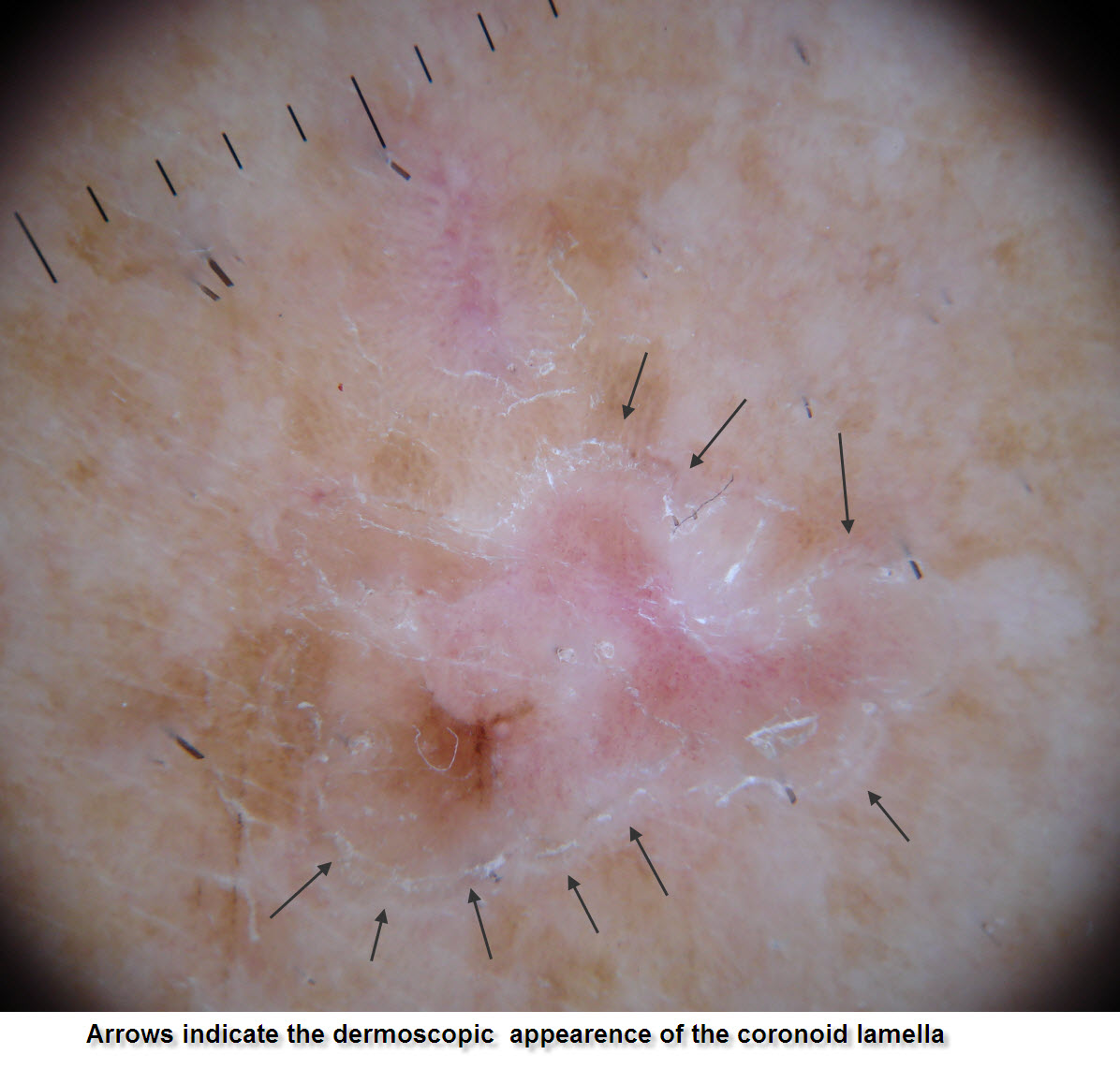
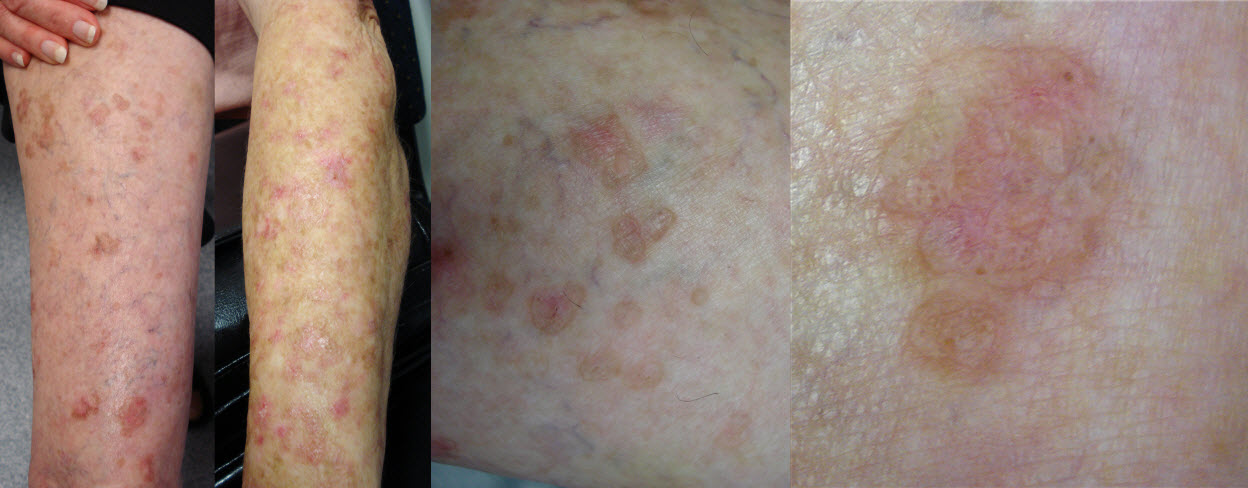
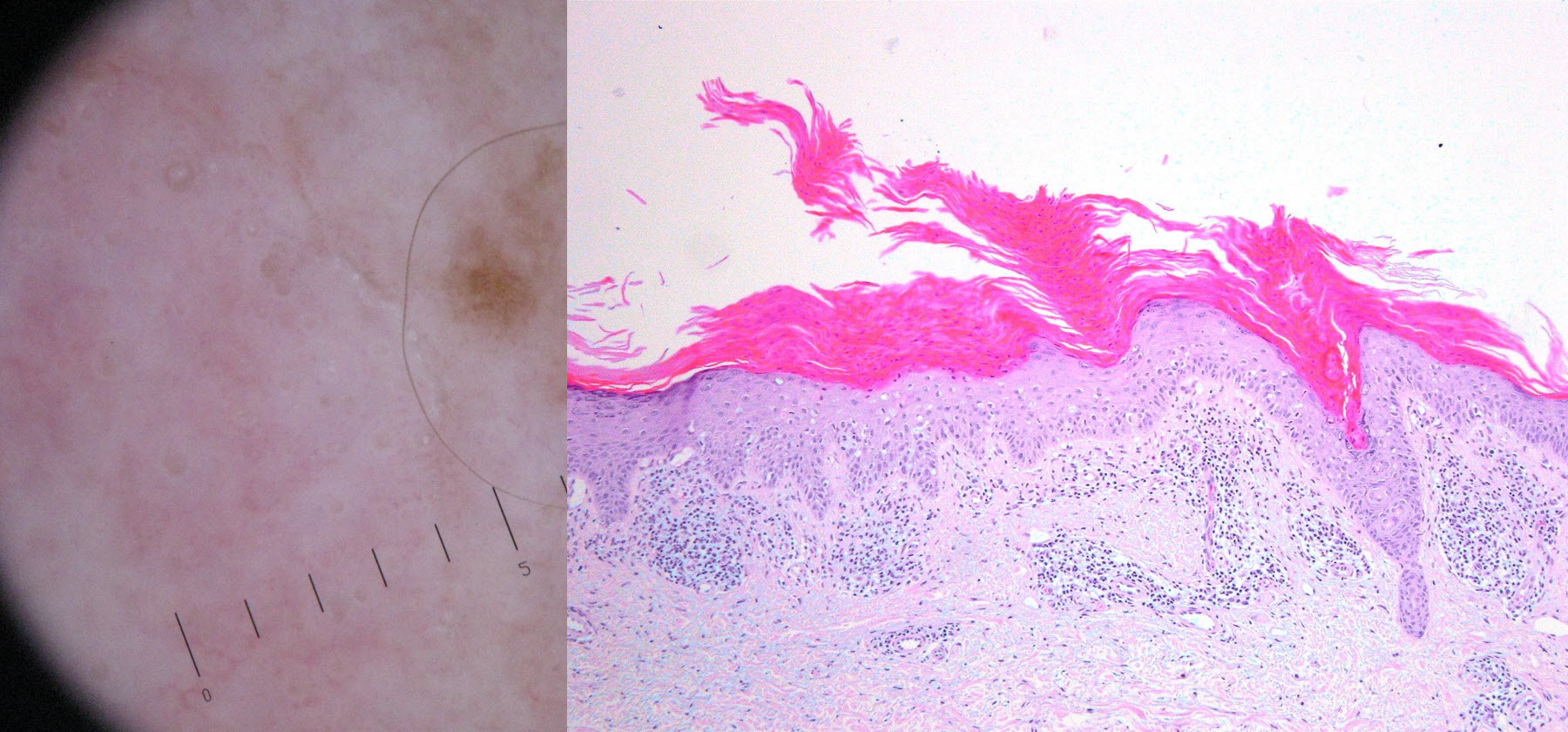
There are actually 3 patient’s presented here a mother and daughter (aged 70's and 40's) with multiple erythrosquamous lesions on the arms and legs, and a third patient (female late 50’s)with a solitary large annular erythrosquamous plaque on the distal triceps. These cases illistrae one the small "s" (solar damage) conditions in the PMsPET pneumonic. The mother and daughter have typical disseminated superficial actinic porokeratosis (DSAP) one of a group of Porokeraoses. The final case is Porokeratosis of Mibelli. . In both clinically the typical finding is an annular rim of keratin scale which histollogically is described as a coronoid lamella. Treatment can be problematic the 2 girls with DSAP have had multiple lesions treated with cryotherapy or Efudix, but other new lesion appear to replace those treated. UV protection is paramount and there is as with solar keratoses a small risk of lesions progressing to IEC/SCC. 80% Liquid phenol apparently works well but I have yet to try this. The isolated Mibelli lesion is being treated with efudix , I will post some follow up images in due course.
|
Related Links: Disseminated superficial actinic porokeratosis Porokeratosis of Mibelli |
|
Case Comments [Add Comment] [Subscribe] |